
Clinician's Guide
to CHL in adults
CHL in Adults
This guide outlines how you can use wideband acoustic immittance (WAI or MEPA) for differential diagnosis of conductive hearing loss (CHL) in adults with an intact tympanic membrane and aerated middle-ear
According to a recent report funded by the NIH (Nakajima et al., 2012), CHL with an intact TM and aerated middle-ear can be associated with three conditions: ossicular fixation (usually from otosclerosis), ossicular discontinuity, and superior semicircular canal dehiscence (SCD). They are sometimes hard to differentially diagnose in the clinic, and may require surgery or expensive tests to fully investigate. Nakajima et al. showed how to use MEPA and an audiogram to aid in the differential diagnosis in an office setting.
This test is applicable to patients with CHL, defined as >10 dB air-bone gap (ABG) on pure-tone audiometry (averaged over either 500, 1000, 2000 Hz or 250, 500, 1000 Hz), and with an intact TM and aerated middle ear.
First, some definitions:
- Absorbance is the inverse of reflectance - it is the amount of power the ear absorbs rather than reflects. It can be specified as a percentage, like reflectance, or it can be converted into a decibel (re 100% absorbance). In the Mimosa Acoustics products and some literature, the decibel version is called Transmittance.
- The absorbance difference level (ADL) plotted by Nakajima, is calculated by subtracting the absorbance (in decibels) from the mean normative absorbance value in the companion paper by Rosowski et al. (2012), which considered normal rather than pathological ears. The ADL averaged over 0.6-1 kHz is the key statistic.
- the ABG is defined as the average between 1 and 4 kHz (this separates out the SCD cases where the ABG is most apparent at frequencies less than 1 kHz).
Interpretation
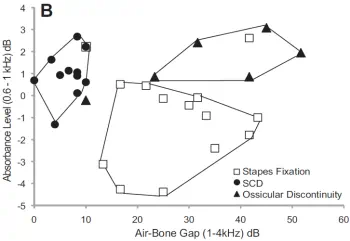
Fig 6B in Nakajima et al. (2012) illustrates how the 3 conditions tend to cluster when plotted as absorbance level difference against the ABG.
To aid in interpretation:
- Ears with ADL (0.6-1kHz) < 1 dB and ABG (1-4kHz) > 10 dB were associated with stapes fixation.
- Ears with ABG (1-4kHz) <= 10 dB were associated with SCD.
- Ears with ADL (0.6-1kHz) >= 1 dB and ABG (1-4kHz) > 20 dB were associated with ossicular discontinuity.
In Nakajima's study, sensitivity and specificity were good (from their Table 1), but they are based on a small number of subjects (N=31 ears), so caution should be used in applying these results:
| Stapes fixation | |
|---|---|
| Sensitivity | 86% |
| Specificity | 100% |
| Ossicular discontinuity | |
| Sensitivity | 83% |
| Specificity | 96% |
| Semicircular canal dehiscence | |
| Sensitivity | 100% |
| Specificity | 95% |
How to run this test
OtoStat 3
- Ensure the patient birthdate is entered accurately in OtoStation.
- Run a MEPA test (or run any non-MEMR test sequence - they all start with a MEPA test).
- Use the dropdown menu on a plot space to choose the Text display, if it is not already showing. The Absorbance Difference Level is displayed in the Text panel if the patient is of adult age.
OtoStat 2.0
- Choose the Adult age-group.
- Make a MEPA measurement and save it. You can optionally continue with the DPOAE measurement, or stop the test early.
- Tap on the screen to advance to the analysis screen, or download to review or print the test in OtoStation. The Absorbance Difference Level is displayed in the analysis panel.
OtoStat R1
- Choose the Adult age-group.
- Make a MEPA measurement and save it. You can optionally continue with the DPOAE measurement, or stop the test early.
- Review the test on your support computer. The Absorbance Difference Level is displayed in the analysis panel.
HearID v3.x, v5.0-5.1
This research was published after HearID's release, so the ADL calculation isn't included in these versions. Subsequent versions of HearID will include the absorbance difference level relative to the specified mean norm. To make this calculation manually:
- Make a MEPA measurement using the default chirp stimulus.
- Export the measurement to an Excel or Matlab file. In the Excel file, look for "powT" (the specific column depends on which other measures are exported). See the MEPA manual for how to export data for offline analysis.
- Calculate the average in Transmittance between 0.6 and 1 kHz.
- Subtract the norm mean (from Rosowski, et al, 2012) of -3.42 dB from your average to get the ADL (or, more simply, add 3.42 to the average).
Further reading
Nakajima, H. H., Pisano, D. V., Roosli, C., Hamade, M. A., Merchant, G. R., Mahfoud, L., Halpin, C. F., Rosowski, J. J., and Merchant, S. N. (2012). "Comparison of ear-canal reflectance and umbo velocity in patients with conductive hearing loss: a preliminary study," Ear Hear. 33, 35-43.
Rosowski, J. J., Nakajima, H. H., Hamade, M. A., Mahfoud, L., Merchant, G. R., Halpin, C. F., and Merchant, S. N. (2012). "Ear-canal reflectance, umbo velocity, and tympanometry in normal-hearing adults," Ear Hear. 33, 19-34.
Keywords
conductive hearing loss, CHL, umbo velocity, middle-ear wideband reflectance, differential diagnosis, semicircular canal dehiscence, superior canal dehiscence syndrome, SCDS, stapedovestibular ankylosis, otosclerosis, stapedectomy.
Disclaimer
This guide was compiled by Mimosa Acoustics from peer-reviewed scientific research (funded by the NIH) to assist clinicians in interpreting results from HearID and OtoStat. It will be updated as new research becomes available. HearID and OtoStat do not provide diagnoses. All diagnostic decisions are the responsibility of the clinician.
Version 1.2, 1 Dec 2024 (updated for OtoStat 3).
Prepared by Judi Lapsley Miller, PhD.
Version 1.0 was reviewed by John Rosowski, PhD, Professor of Otology and Laryngology, Massachusetts Eye and Ear Infirmary, 9 July 2013.