
Clinician's Guide
to ME effusion in children
Identify MEE in children
Middle-ear effusion (MEE) and negative middle-ear pressure tends to stiffen the middle ear and thereby increase the amount of energy reflected, particularly around 1-3 kHz, compared to normal ears. This increased reflectance can be used to identify MEE in children.
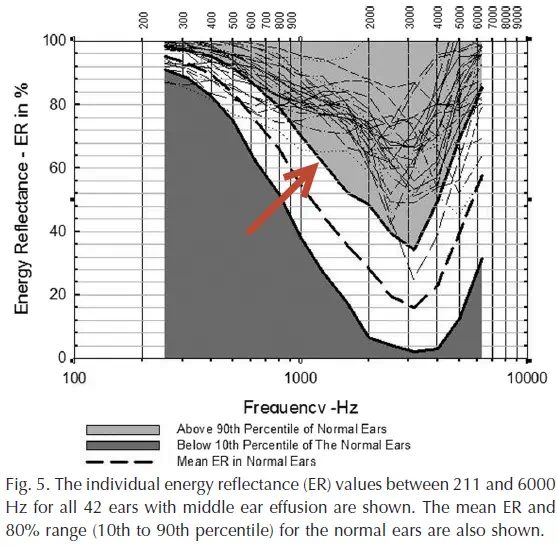
Beers et al. (2010) tested 78 children (144 ears) with normal middle ears and 64 children with abnormal middle ears (42 ears with MEE and 54 ears with negative middle-ear pressure) using wideband reflectance. The children were aged 5-7 years. They found that reflectance in the frequency region around 1.25 kHz best separated the normal ears from those with MEE.
Using the 90th percentile from the normal group as a criterion, all ears with MEE had higher reflectance than the criterion at 1.25 kHz (hit rate 100%), for a false-alarm rate of 10%. They also showed that reflectance was much more sensitive than 226 Hz tympanometry in detecting MEE.
On average, ears with negative middle-ear pressure had higher reflectance than normal, but not as high as those ears with MEE.
Interpretation
Use the Reflectance Area Index (RAI) for the 1/3rd octave around 1.25 kHz for the chirp stimulus. The RAI is the average reflectance across a frequency region.
- An RAI ≥ 62% is consistent with middle-ear effusion in children aged 5-7 years.
- An RAI < 62% is consistent with a nomal middle ear in children aged 5-7 years.
How to run this test
OtoStat 3
- Ensure the patient birthdate is entered accurately in OtoStation.
- Run a MEPA test (or run any non-MEMR test sequence - they all start with a MEPA test).
- Use the dropdown menu on a plot space to choose the Text display, if it is not already showing. The RAI and Beers' summary is displayed in the Text panel if the patient is a child.
OtoStat 2.0
Ensure the "MEPA chirp 60" protocol is selected. The MEPA and DPOAE test are run automatically and displayed on-screen together when choosing the "Child 3-16y" button. If you are solely interested in reflectance, you can stop the test early before the DPOAE test is run.
Tap on the screen to advance to the analysis screen, or download to review or print the test in OtoStation. The RAI (1.25kHz) is displayed. On the print summary, Beer's criterion for MEE (above) is also included for comparison.
OtoStat R1
Ensure the "MEPA chirp 60" protocol is selected. The MEPA and DPOAE test are run automatically and displayed on-screen together when choosing the "Child 3-16y" button. If you are solely interested in reflectance, you can stop the test early before the DPOAE test is run.
On the print summary, the RAI (1.25kHz) is printed out along with Beer's criterion for MEE.
HearID v3.x and v5.x
- For MEPA, use the default chirp stimulus and run the test.
- Export the data (see manual) and open in Excel. Find the column "energyReflectance" and take the average between 1122 and 1414 Hz. This is the one-third octave RAI around 1.25 kHz.
Further reading
Beers, A. N., Shahnaz, N., Westerberg, B. D., and Kozak, F. K. (2010). "Wideband reflectance in normal Caucasian and Chinese school-aged children and in children with otitis media with effusion," Ear & Hearing, 31, 221-233.
Hunter, L., and Shahnaz, N. (2013). Acoustic Immittance Measures: basic and advanced practice. (Plural, San Diego, CA).
Keywords
otitis media, otitis media with effusion, MEE, OME, OM, wideband reflectance, tympanometry, child, norms, middle ear.
Disclaimer
This guide was compiled by Mimosa Acoustics from peer-reviewed scientific research to assist clinicians in interpreting results from HearID and OtoStat. It will be updated as new research becomes available. HearID and OtoStat do not provide diagnoses. All diagnostic decisions are the responsibility of the clinician.
Version 1.2, 1 Dec 2024 (updated for OtoStat 3).
Original version 1.0, 5 July 2013.
Prepared by Judi Lapsley Miller, PhD.